
How Our Videos Are Made
A Visual Journey Behind the Scenes
Bringing Care to Life
We developed our production process to meet the specific and special needs of clinical teaching videos. We show accurate, up-to-date standards of care that are relevant to the realities of working in low-resource settings – and highlight the human aspect of respectful care.
We aim to create videos that are clear, accurate, and practical. Though they may appear short and basic, lots of planning and effort goes into achieving that brevity and simplicity.
Curious about what happens behind the scenes?
Scroll down for a journey through the process we’ve developed.

The Planning Phase
First we choose a series of videos where we think we can make a difference: an urgent global health issue that can be taught well with video – within a group of micro-topics.
Once the broad topic is decided, there’s a lot to do before we ever set foot on a shoot.
Scripts are written for each topic based on the latest guidelines and relevant resources. They are rigorously reviewed by our team of global content experts and revised as needed. Scripts are our roadmap and our guide to filming.
Shot lists are developed next. They answer the question, “What are we seeing as we are saying that?”
We imagine exactly what the health worker is doing, and what else is in the scene, anticipating needed supplies before arriving on a shoot. We bring items with us that may not be available at the film location; for example, resuscitation equipment, baby hats, and sterile gloves.

We also answer some seemingly mundane, but important questions. For example: do health workers need to wear gloves for this procedure? And, if so, must they be sterile or can they be clean exam gloves?
Gloves are scarce in resource-limited settings and often need to be washed and sterilized between uses.

The Film Sites
We find two or three film sites (on different continents) because it is seldom possible to get all the needed footage in one location, and we aim to have a diversity of people and cultures in our videos.
It‘s important that health workers relate to the setting in the films so we look for a low-resource environment.
A site visit before filming is always valuable, if we have the budget. We meet the host team, tour the facility, and assess the filmmaking needs for lighting, equipment, and props.

Once our scripts are ready and the clinical site is chosen, we’re ready to travel. We go with a small, dedicated team – our medical director/producer and two videographers.
We pack the equipment we need to shoot quality footage, that is also portable and durable enough for the unpredictability of our locations. We pack plenty of batteries, odds and ends for repairs and to attach our lights to ceilings and walls, plus props for all the details we’ve anticipated.
We max out our baggage allowance with gifts for the people in our videos – often baby clothes that are donated by a local children’s store.


Once on site, we choose the health workers who will participate in the videos.
This is a key to our success. The health workers must be skilled as well as confident, comfortable and natural in front of the camera. Quality of care includes kindness and respect – so they need to have a naturally warm, kind and caring attitude with people.
We are grateful to have worked with dozens of exceptional health workers all over the world.



We’re resourceful in turning almost any room in a facility into a temporary film studio.
The environment should look modest, like a clinic room anywhere in the developing world – and clean.

We work on location for 2-to-3 weeks, filming every day, and filming everything we can from our long shot list. We review footage in the evenings so we know what we’ve gotten and what remains to be filmed, or filmed again.
We always get verbal and written permission from the people in our films. Women are often happy to participate in filming that will help other women and babies get better care – and it’s OK if she changes her mind.




Teaching films need to be uncompromisingly accurate and the practices need to follow up-to-date international guidelines. Even though our health workers are skilled and competent, filming almost always involves coaching clinical practices during the shoot.



Back Home, the Videos Come Together
The footage is reviewed and the best shots are selected. We adapt the narration to closely relate to the action in the footage; bringing the teaching points to life. We use an active voice and simple language.
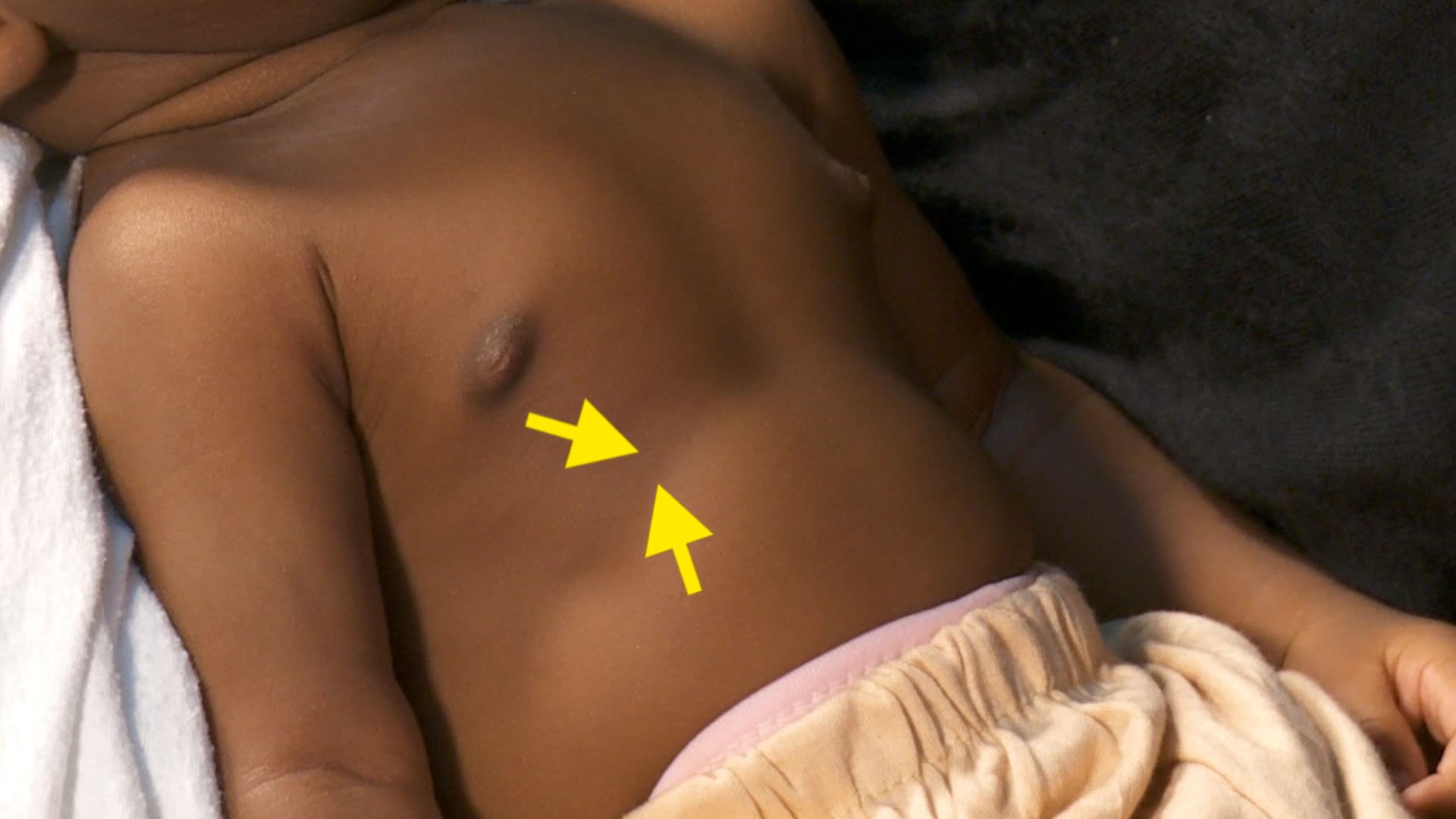
Where we anticipate the learner will need more visual explanation, we use graphics to direct the eye, side-by-side comparisons, and image overlays to show what’s happening inside the body.

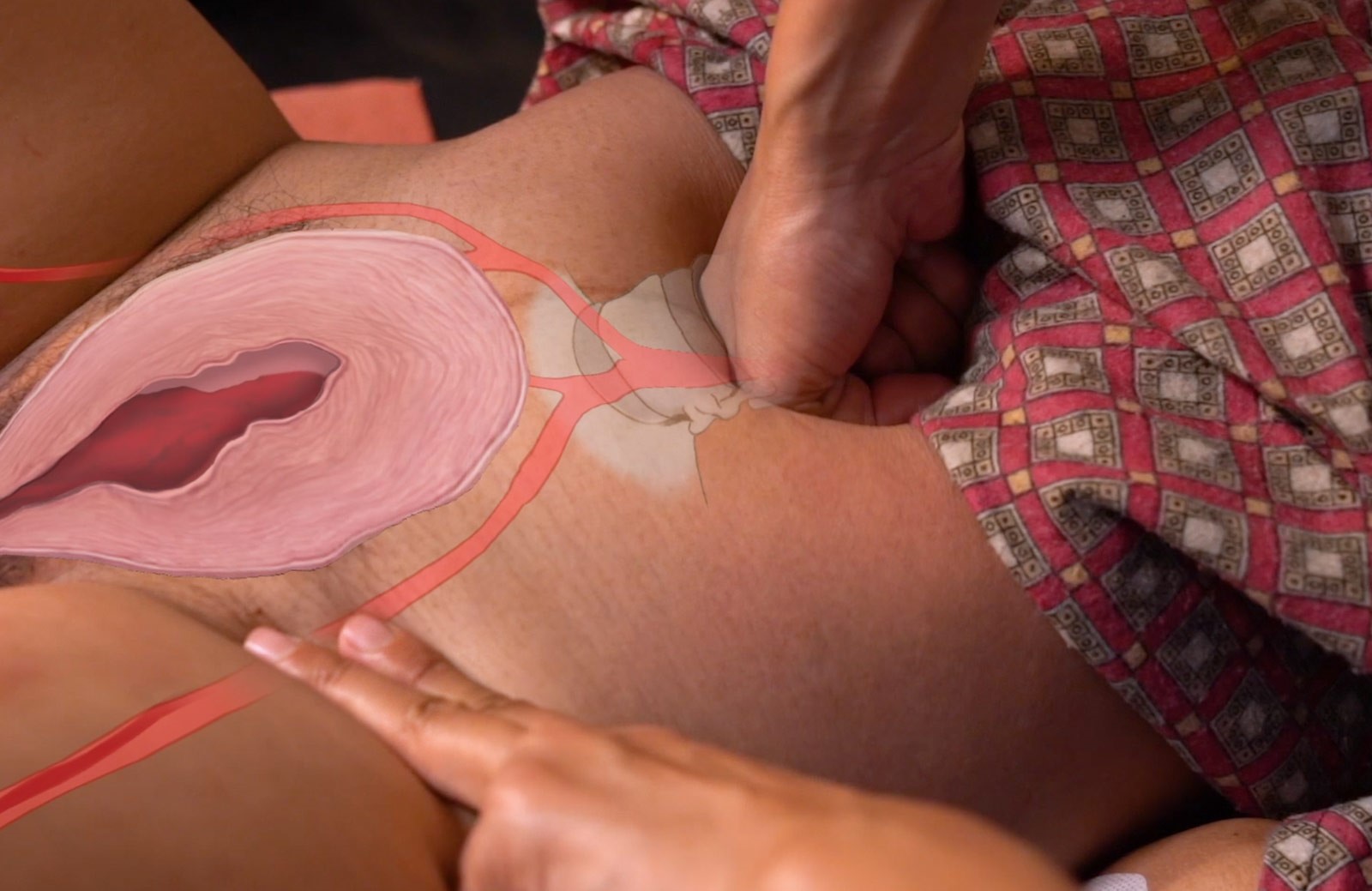

We also create graphics and animation to unpack a procedure or see inside the body to explain the how and why of skills and practices. This involves hand-drawing step-by-step storyboards and continual communication with the artist animator.


Our draft videos are sent to our content experts for review, then they are revised as needed. The videos are finalized with color correction, audio work, and final narration in English, French and Spanish. They have a final review by our team of non-medical folks to be sure the videos are simple enough to follow even by untrained people.


Final videos are then uploaded to the internet for streaming and compressed into convenient sizes for download worldwide.
Most of our languages are translated and narrated through the extraordinary collaboration of individuals and organizations across the globe who reach out to us and do the work voluntarily. Please contact us if you would like to narrate our videos in your language.
The videos are used by 1000s of organizations and health workers worldwide – in face-to-face workshops, distance learning courses, hospital waiting rooms, and on phones, right in the palm of the hand.

